Health
Ambient AI scribes spread in clinics, raising accuracy concerns
The new bargain in exam rooms is simple and uneasy: let AI handle the notes, and physicians may have more time to look patients in the eye. The catch is that a live microphone is now capturing some of the most intimate conversations in medicine, from symptoms and medications to consent language and side discussions that were never meant for a second set of ears.
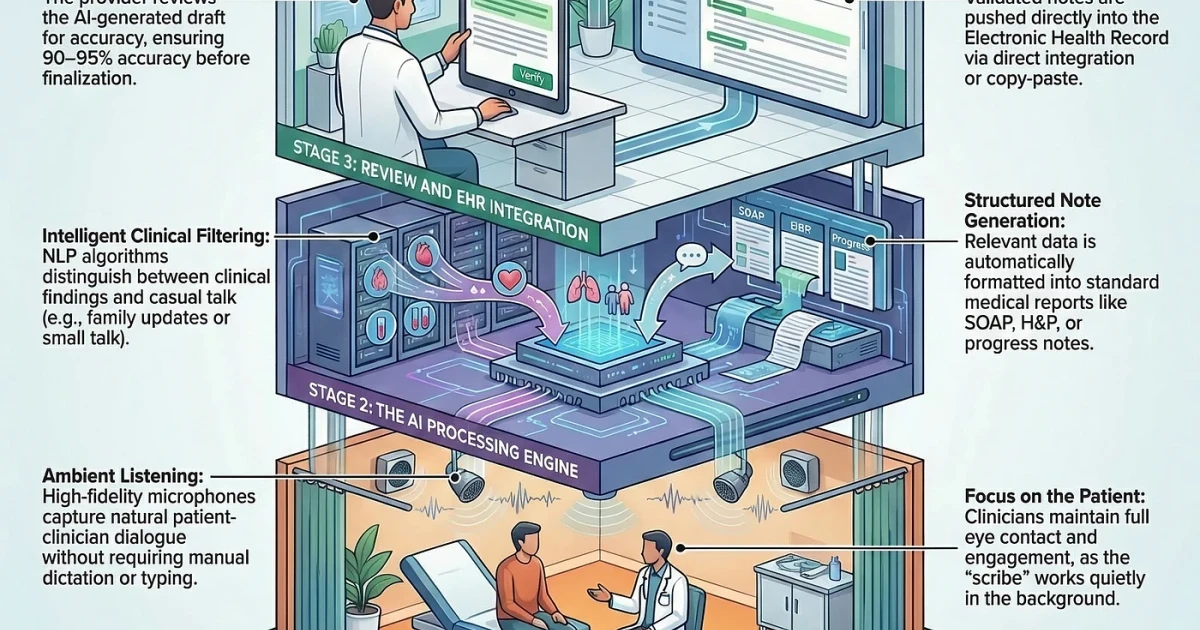
Medscape’s Scribe product shows why clinics are moving quickly. The system listens during patient visits, generates an EHR-ready summary, lets the clinician edit it, and then transfers the note into the chart. Medscape describes the tool as HIPAA-compliant, available only in the United States, and set to delete transcripts and summaries after 72 hours. That promise of less documentation burden has made ambient AI especially attractive to physicians pressed by long days and rising paperwork.
But the technology’s appeal is also what makes it risky. If the system mishears a medication name, flattens a symptom description or misses the language around consent, the final record can carry an error into future care. The clinician remains responsible for the chart even when AI drafted the first version, which means the legal and professional burden does not disappear when the note is automated.
A JAMA Network Open quality-improvement study offers a closer look at how patients and clinicians are handling that shift. Among 121 pilot users, including 18 clinicians and 103 patients, the most common approach to consent was a verbal patient-clinician conversation before the encounter. Comfort with the tool varied depending on trust in the clinician, understanding of how the system worked and whether patients saw more benefit than risk. Participants wanted something more flexible, including education, digital resources, help from nonclinical staff and an opt-out option.

The stakes are already reaching the courtroom. A proposed class-action lawsuit against Sharp HealthCare in San Diego, California, alleged that an AI-powered ambient documentation tool recorded doctor-patient conversations without proper consent and falsely documented consent in the chart. That dispute underscored how quickly the software has moved into practice, and how slowly policy has caught up.
The efficiency case is strong. The American Medical Association said The Permanente Medical Group used ambient AI scribes 2.5 million times in one year. Kaiser Permanente reported nearly 16,000 hours of documentation time saved over 15 months, and a TPMG analysis said the system saved the equivalent of 1,794 working days over 63 weeks. It also reported better physician-patient communication. Yet those gains now sit beside harder questions about regulation, accuracy and who is accountable when a machine gets the medical record wrong.