Health
Ebola outbreak widens in DRC as scientists race to test treatments
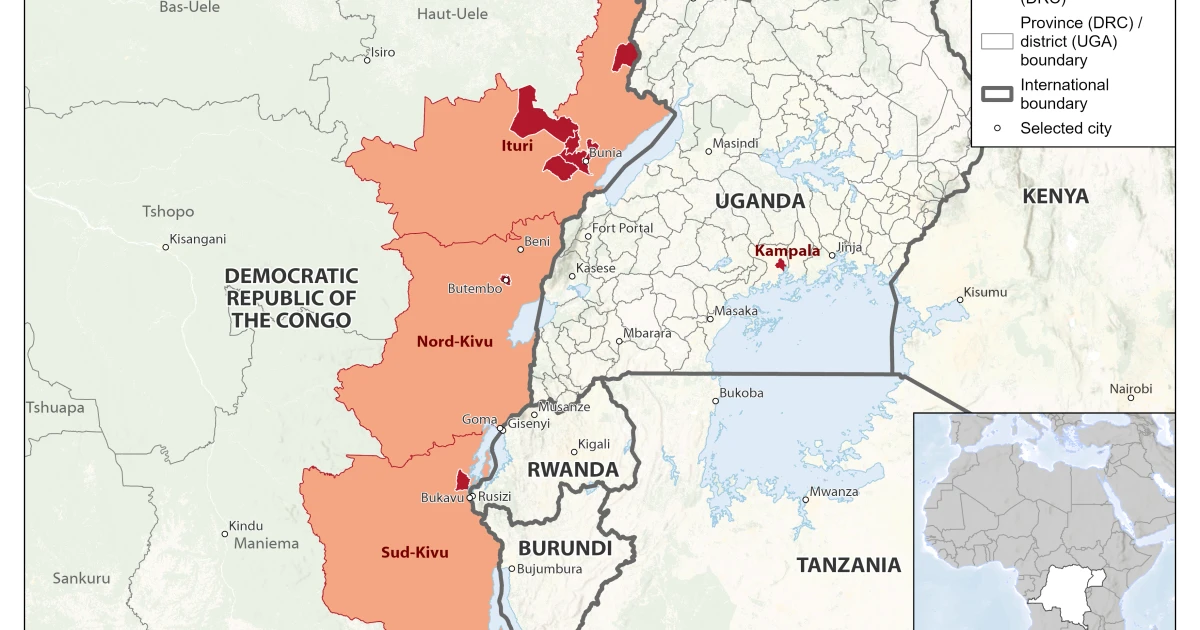
A fast-moving outbreak of Bundibugyo virus disease has widened in eastern Democratic Republic of the Congo and crossed into Uganda, exposing how little proven medical firepower exists against one of Ebola’s least studied strains. By June 2, the U.S. Centers for Disease Control and Prevention said the outbreak had reached 378 confirmed cases and 63 confirmed deaths across the two countries, while still noting on June 12 that no Ebola cases had been confirmed in the United States and the risk to the American public remained low.
The outbreak was first flagged on May 5, when the World Health Organization received an alert about a high-mortality illness in Mongbwalu Health Zone in Ituri Province. After testing 13 samples from Rwampara Health Zone and finding eight positive, WHO confirmed Bundibugyo virus disease on May 15, the same day Congo’s health ministry declared the country’s 17th Ebola outbreak and Uganda confirmed a linked imported case. WHO then declared a Public Health Emergency of International Concern on May 17, after officials had already reported eight laboratory-confirmed cases, 246 suspected cases and 80 suspected deaths in Ituri Province.
The scientific challenge is stark: Bundibugyo virus disease has no licensed vaccine or specific approved therapy. On May 28, WHO expert groups said candidate products should be used only in clinical trials and prioritized MBP134, maftivimab and remdesivir for evaluation, while identifying obeldesivir as a priority candidate for post-exposure prophylaxis research. WHO and outside experts also reviewed Ervebo, the licensed Ebola vaccine used against other Ebola strains, but concluded that evidence for protection against Bundibugyo remained limited and inconclusive.

That uncertainty is driving a race to develop new countermeasures. The Coalition for Epidemic Preparedness Innovations has fast-tracked three investigational Bundibugyo vaccine candidates from IAVI, Moderna and the University of Oxford, with manufacturing support from the Serum Institute of India and funding reported at roughly $60 million. The effort underscores how a rare virus first identified in Uganda in 2007, and seen again in Congo in 2012, can still outpace the global system built to stop it.
The response has also been shaped by the realities on the ground in Ituri, where insecurity, cross-border movement and fragile health services complicate contact tracing and safe burials. The International Federation of Red Cross and Red Crescent Societies said three Congo Red Cross volunteers from the Mongbwalu branch died during the response period, a grim reminder of how quickly responders can become victims when a virus is not yet identified.

CDC says Bundibugyo ebolavirus has caused death in about 30% of infections, with earlier outbreaks showing mortality between 25% and 50%. After Covid, the test is no longer whether the world can name the threat; it is whether trials, stockpiles and border health systems can move fast enough when a rare strain begins to spread.
Sources
- [1]news.google.com
- [2]who.int
- [3]cdc.gov
- [4]cepi.net
- [5]ifrc.org