Health
First-ever guideline targets cardiovascular-kidney-metabolic syndrome screening and treatment
Primary care visits for adults and children with excess weight are set to change. The new cardiovascular-kidney-metabolic guideline tells clinicians to look earlier for excess or dysfunctional adiposity, abdominal adiposity, abnormal lipids, high blood glucose and reduced kidney function, then manage those risks as one connected syndrome instead of separate problems.
The American Heart Association and the American College of Cardiology issued the first-ever clinical practice guideline for cardiovascular-kidney-metabolic syndrome on June 9, 2026, with endorsement and collaboration from the American Diabetes Association and the American Society of Nephrology. Published in Circulation and the Journal of the American College of Cardiology, it replaces and expands the 2013 AHA/ACC/TOS guideline on overweight and obesity in adults.
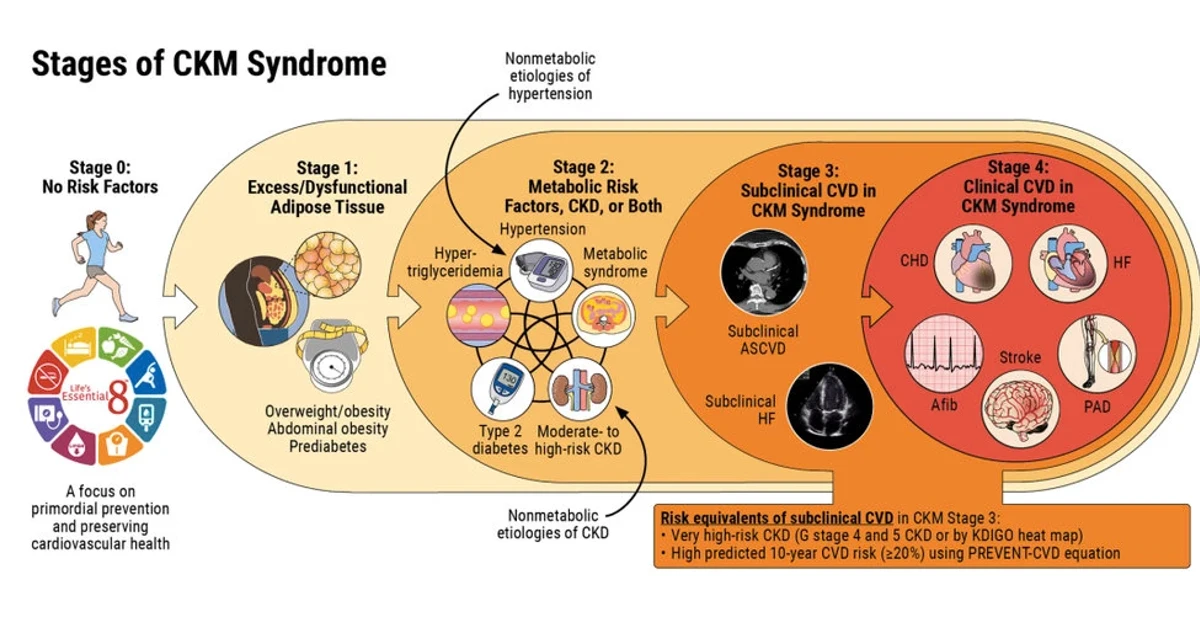
The societies are casting the problem as broad and immediate. The American Heart Association says nearly 90% of U.S. adults have at least one CKM risk factor, and that 40% of U.S. adults and 21% of U.S. children and adolescents have obesity. The new framework runs from Stage 0, with no CKM risk factors, through Stage 4, clinical cardiovascular disease. Stage 1 centers on excess or dysfunctional adiposity; Stage 2 includes metabolic risk factors or moderate- to high-risk chronic kidney disease; and Stage 3 covers subclinical cardiovascular disease or high-risk equivalents.
For a standard visit, the guideline pushes a more structured workup. Adults at risk in stages 0 through 3 should have their cardiovascular risk quantified with the PREVENT equations, which estimate 10-year and 30-year risk for atherosclerotic cardiovascular disease, heart failure and total cardiovascular disease. A predicted 10-year cardiovascular risk of at least 20% is one criterion for Stage 3, while 7.5% or greater helps prioritize pharmacotherapy. The guideline also calls for routine assessment of overweight and obesity, abdominal adiposity, metabolic risk factors and kidney function, with selected checks for pre-heart failure, MASLD and obstructive sleep apnea.
Treatment is meant to be stepped up earlier, not delayed until disease is advanced. The recommendations include lifestyle change, GLP-1-based therapies, SGLT2 inhibitors and, when appropriate, metabolic and bariatric surgery. The document also urges interdisciplinary care, including a CKM coordination point person for patients who have overlapping type 2 diabetes, chronic kidney disease and cardiovascular disease, along with screening for social determinants of health that can worsen CKM burden and outcomes.
Chiadi E. Ndumele, who chaired the writing committee, called CKM a “real, rising public health threat.” The message from the new guideline is clear: excess weight is no longer being treated as a cosmetic issue or an isolated risk factor, but as an early entry point into a disease pathway that can damage the heart, kidneys and metabolism together.
Sources
- [1]news.google.com
- [2]newsroom.heart.org
- [3]professional.heart.org
- [4]heart.org
- [5]tctmd.com