Health
What I wish I knew at 13 about cannabis and long-term risks

The legalization era has made cannabis feel ordinary, but ordinary does not mean harmless. The clearest public-health message is the one too many adolescents still do not hear early enough: the brain is still developing, high-frequency use can become dependency, and the risks do not end when the high fades.
The numbers start young
Cannabis use is not confined to adulthood, and the school years are where the pattern often takes hold. The Centers for Disease Control and Prevention says that in 2022, 30.7% of U.S. 12th graders reported cannabis use in the past year, and 6.3% reported daily use in the past 30 days. Columbia University Irving Medical Center also pointed to earlier exposure, noting that 2019 data showed 37% of U.S. high school students had tried or used marijuana at least once and 22% had used it in the previous 30 days.
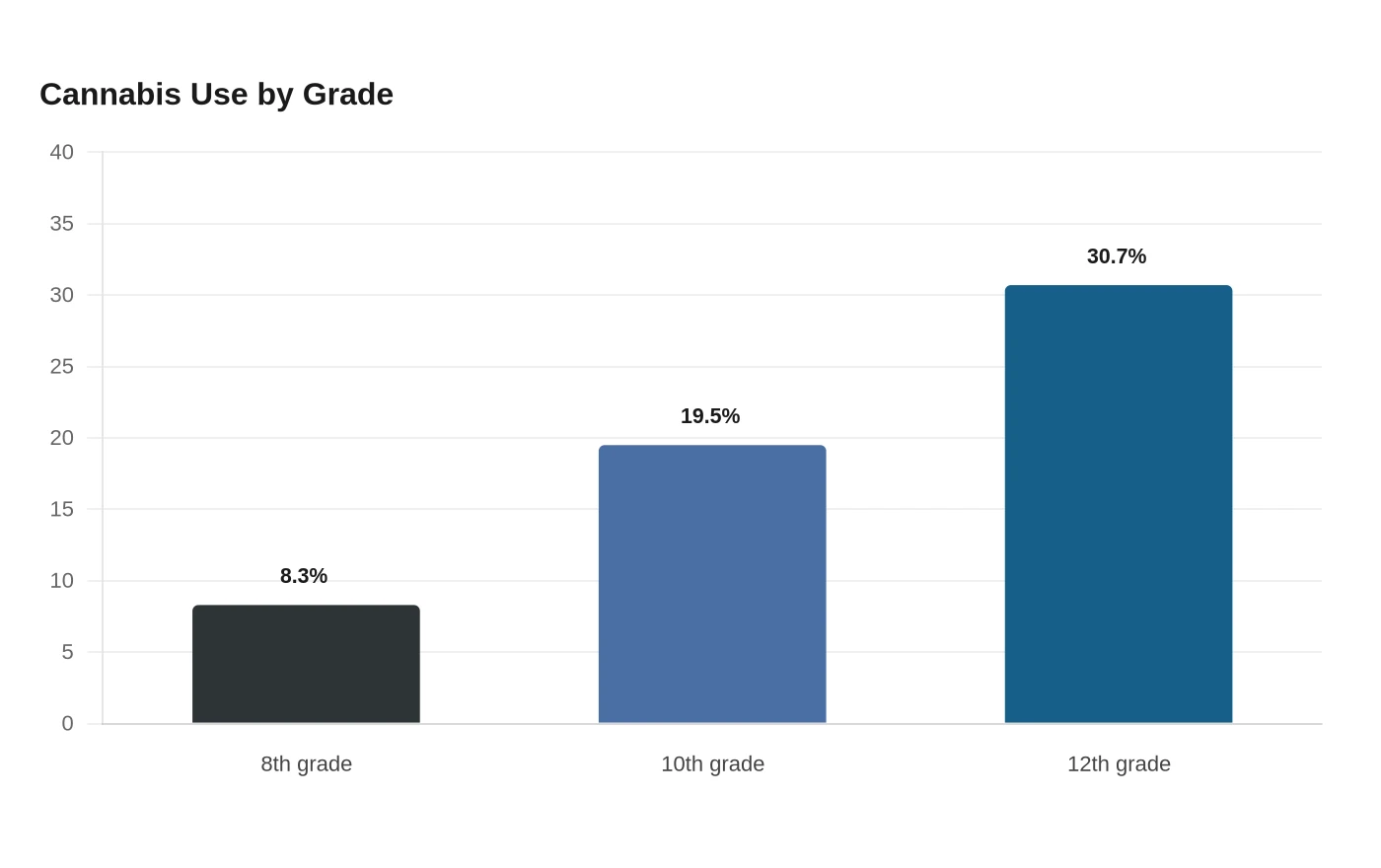
The trend rises sharply by grade. Columbia’s 2022 figures show 8.3% of eighth graders, 19.5% of 10th graders, and 30.7% of 12th graders using cannabis, a staircase that tracks how quickly experimentation can become routine before adulthood. Those numbers matter for schools, pediatric clinics, and families because they show that prevention has to begin well before the final years of high school.
A brain still under construction
The CDC says the teen brain continues developing until around age 25, which is why adolescence is not just another phase of use. Cannabis use during that window may harm the developing brain, and the CDC links it to problems with memory, learning, attention, coordination, school performance, and social life.

Dependency is part of the picture too. The CDC says about 3 in 10 people who use cannabis develop cannabis use disorder, and the risk is higher for people who start in youth. That is the public-health reality behind casual language about “just weed”: for a significant share of users, repeated exposure can move from recreation to compulsion, with consequences that spill into school attendance, family relationships, and mental health care.
What larger studies are finding
The strongest warning signs are showing up in population studies, not just anecdotal accounts. In a Kaiser Permanente Northern California cohort led by Kelly C. Young-Wolff and colleagues, researchers followed 463,396 adolescents ages 13 to 17 who were screened between 2016 and 2023. The analysis, conducted from February 21, 2024 to August 27, 2025, found that past-year cannabis use was associated with increased risk of incident psychotic, bipolar, depressive, and anxiety disorders by age 26.
That study adjusted for sex, race and ethnicity, neighborhood deprivation index, insurance type, and time-varying alcohol and other substance use, which makes the signal harder to dismiss as a simple byproduct of other risks. It does not mean every teen who uses cannabis will develop a psychiatric disorder, but it does mean the idea that adolescent use is low-stakes is not supported by the evidence.
A separate Johns Hopkins Bloomberg School of Public Health analysis of nearly 700,000 health records sharpened the concern for younger users. Among young people 17 and under with cannabis use disorder, the relative risk was 52% higher for schizophrenia, 30% higher for recurrent major depression, and 21% higher for anxiety disorders compared with young people with other substance use disorders. That comparison is especially important because it places cannabis disorder alongside other serious substance-use conditions instead of treating it as a minor side issue.
Legalization changed access, potency, and expectations

Cannabis did not emerge from nowhere with legalization. Johns Hopkins notes that it has been used recreationally in the United States since at least the 1800s, became more popular during alcohol prohibition in the 1920s, and surged again during the counterculture movement of the 1960s. What is different now is the scale of legal access: adult use is legal in 24 U.S. states and the District of Columbia.
Columbia University Irving Medical Center said that as recreational legalization expanded, product potency increased and the risks for teenagers changed. That shift matters because today’s products are not the same as the lower-potency cannabis many adults remember from decades ago. For teens, the combination of easier access, stronger products, and social normalization can make risky use look invisible until school problems, anxiety, or dependence become impossible to ignore.
What honest education should cover
The gap is not only in knowledge, it is in the conversations adults avoid. Columbia’s guidance is direct: talk to teens, because silence can do more harm than guidance. That means replacing vague warnings with specifics about age, dose, frequency, and mental health, instead of assuming that a legal product is automatically safe for a developing brain.
• Say plainly that the brain is still developing until about age 25.
• Name the dependency risk, especially if use starts in adolescence.
• Explain that daily or near-daily use is not the same as occasional experimentation.
• Connect cannabis to school, memory, attention, and social functioning, not just to intoxication.
• Treat anxiety, depression, paranoia, and sleep disruption as reasons to pause, not as side effects to shrug off.
The legalization era has changed the social script around cannabis faster than it has changed teen education. The public-health task now is not to moralize about use, but to tell young people the truth early enough that they can make a real choice before dependency, potency, and psychiatric risk narrow the options.