Health
Why U.S. measles outbreaks are getting harder to stop
The United States declared measles eliminated in 2000, meaning there was no continuous domestic transmission for 12 months or more. But the virus never left the picture completely. A single imported case can still seed a chain of infections in communities where vaccination coverage has slipped below the level needed to hold the line.
Elimination did not mean immunity from outbreaks
The central weakness in the current system is not that measles returned, but that many places no longer have the vaccination cushion that once stopped it. About 95% two-dose coverage is needed for herd immunity, and the CDC warns that measles can spread in any community that falls below that mark. That leaves schools, clinics, and neighborhoods exposed whenever a case is brought in from outside the country or from another part of the United States.
That reality is why elimination status can coexist with recurring outbreaks. The designation means the virus is not continuously circulating across the country, not that every county is protected. When importations land in a pocket of low coverage, the response is no longer a matter of isolating one sick patient. It becomes a race to find every exposed person before the virus moves through households, classrooms, waiting rooms, and faith or social networks.
The numbers show a system under strain
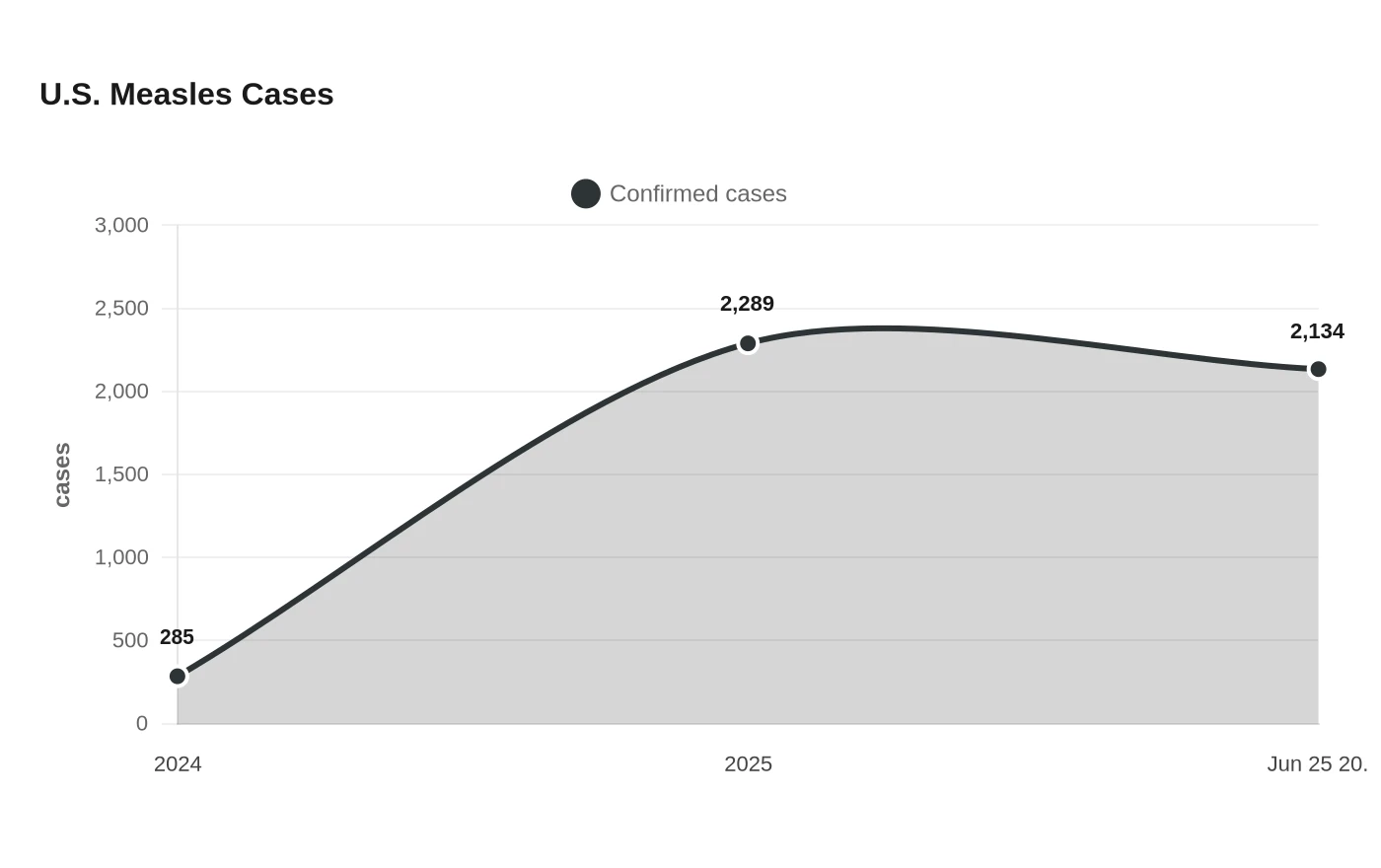
The outbreak record has worsened sharply. The CDC reported 2,289 confirmed measles cases in 2025, with 48 outbreaks and 90% of cases tied to outbreaks. That was a major jump from 2024, when the country recorded 285 cases, 16 outbreaks, and 69% of cases associated with outbreaks. By June 25, 2026, the U.S. had already logged 2,134 confirmed cases, a pace that put the country on track to match or exceed the 2025 total.
The disease keeps finding openings. The CDC counted 26 cases among international visitors in 2025, a reminder that importations remain part of the equation even when domestic transmission is interrupted. Public-health experts have long treated that as the predictable pressure point: measles does not need many chances, only one susceptible cluster.
The 2025 U.S. case count was the highest since 1992, and Stanford Medicine researchers warned that if immunization levels stay where they are, measles could become endemic in the United States within two decades.
West Texas showed how fast an outbreak can outgrow the first case
The largest 2025 outbreak began in west Texas and spread across close-knit communities in Texas, New Mexico, and Oklahoma with low vaccination coverage. From January 1 to April 17, 2025, the CDC counted 800 U.S. cases, with 82% linked to that ongoing outbreak. In the same period, 85 patients were hospitalized and three died.
The outbreak kept growing. In a separate CDC analysis of the South Plains region of west Texas, 325 cases were reported in the first three months, from January 20 through March 18, 2025, and 60 patients were hospitalized. Texas later reported that the outbreak had reached 762 confirmed cases and 99 hospitalizations before being declared over on August 18, 2025.
Measles is so contagious that once it enters a vulnerable community, public health has to move immediately on case finding, exposure notification, isolation, and vaccination. If coverage is already thin, every delay enlarges the circle of people who need tracing and every missed exposure increases the odds that the next case will appear somewhere else.
Why the outbreak model is getting harder to break
The virus’s extreme contagiousness is only part of the problem. The other part is structural: missed immunizations after the pandemic, uneven local coverage, and the reality that imported cases do not have to travel far to find people who can still catch measles. Declining vaccination rates and the rebound of missed childhood immunizations have left more children susceptible worldwide, increasing the chance that imported cases will ignite outbreaks in the U.S.
The failure point is a public-health system that depends on uniform coverage but now has to operate across patchy immunity, multiple jurisdictions, and communities that may not register the first case quickly enough to stop spread. Johns Hopkins’ International Vaccine Access Center identified west Texas as the center of the largest current outbreak before it spread outward from there.
What this means for schools, clinics, and local health departments
In practical terms, the containment model breaks first in the places that see people before anyone knows measles is present. Schools have to manage exposures, verify immunization records, and exclude unvaccinated students when necessary. Clinics face the challenge of identifying suspected cases quickly, preventing waiting-room spread, and protecting infants, cancer patients, and others who cannot be vaccinated. Local health departments must then absorb the labor-intensive work of tracing contacts, coordinating testing, and issuing guidance fast enough to matter.
That burden falls hardest on departments with limited staff and limited room for error. A few linked cases can consume the same response machinery that would normally handle many smaller public-health events, especially once the caseload rises into the hundreds, as it did in Texas and across the national tally in 2025.
Sources
- [1]news.google.com
- [2]cdc.gov
- [3]dshs.texas.gov
- [4]publichealth.jhu.edu
- [5]who.int